While I never watched a full episode of Game of Thrones, I’m familiar with the ominous warning that “winter is coming…”
If you’re involved in the health system as a consumer or community representative, then you’ll know that health services in the south of the state are battening down the hatches to prepare for the increase in people who get sick at this time of year.
But we know from our discussions with WA community members that people don’t want to get sick if they can help it. Getting sick during winter isn’t inevitable and we know that every time you get a group of health consumers in a room, people sharing their knowledge is powerful.
So while we couldn’t easily get almost 200 people together in a room, we’ve gathered views from 200 of you about how you stay well and if you’re stepping up your efforts as winter approaches. Here’s what you told us…
First up – you care about your health
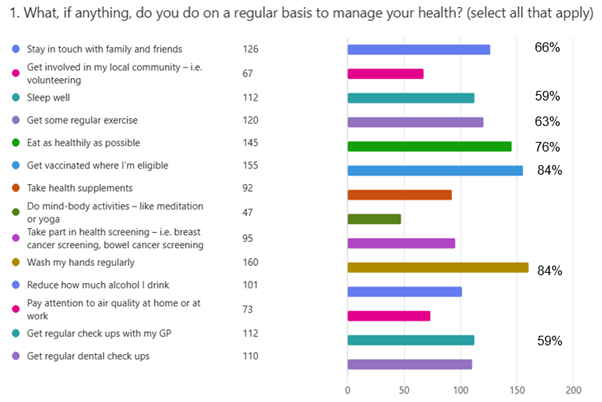
Everyone does something to protect their health usually. With the most selected options being:
Wash hands
Get vaccinated
Eat as healthily as possible
Stay in touch with family and friends
Get some regular exercise
Getting regular check ups with your GP and sleeping well scored highly too.
Next – most of us are doing something extra to prep to avoid winter bugs
More than three quarters of respondents think about taking extra measures – including:
Getting vaccinated
Maintaining strong hygiene like hand-washing and using masks
Avoiding higher-risk environments during peak season
Staying home and keeping your distancewhen unwell
Building overall health and immunity
Paying attention to air quality and ventilation
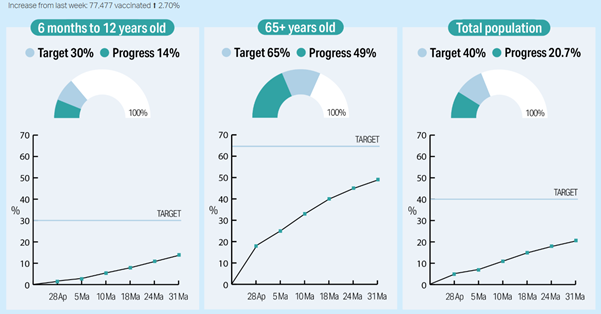
Most of our respondents plan to get vaccinated if they’re eligible
More than 80% of respondents plan to get vaccinated and know where to go to get it done, with about 7% of respondents unsure. Among the people who say they’re not planning to get vaccinated, about 5 people express concern about the risks of vaccination, with another 7 people commenting on how they’ve experienced cold/flu-like illnesses after previous vaccinations.
We can all play our part in reaching the community target which gives us all the best chance of staying safe. At the time of writing we’re already over half way towards these targets – but there’s still a way to go. You can check out progress at the WA Health site here: https://access.health.wa.gov.au/immunisation
Finally, we want clear, accessible public health information in places where we already go
People also said they want strong public health messaging and transparency – if you haven’t already, check out the WA Health website which has links to your nearest place to get vaccinated, as well as more information about what to expect.
Survey information
We shared a link to a MS Forms survey between 06/03/26 and 09/06/26. The link was shared with HCCWA networks via email and social media. It was also shared on Reddit in r/Perth. There were 191 respondents. Over three quarters of respondents belong to a group that is known to experience health inequities. Almost a quarter of respondents were between 35-44, and over one tenth of respondents were 75 or over.
An essential building block of clinical governance working under the radar.
Individual health advocacy places the person at the centre of care and decision-making about their healthcare. In a busy and highly fragmented health system, independent health advocacy is a critical part of the safety and quality landscape. Health systems are stronger and safer when people are heard, respected and supported in decision-making. The ability to access independent individual advocacy support can help to restore people’s trust in the health system and rebuild their confidence to speak up in future.
Unprecedented increase in need
We are experiencing unprecedented levels of IHAS need for specifically ‘in-the-moment’ advocacy cases from Western Australians.
Category 1 cases aim to be attended to within 24 to 48 hours due to crisis or life altering impact.
January to March 2026 saw an 111% increase in Category 1 cases compared to January to March 2025.
111%
↑ category 1 cases
Our impact by the numbers
Enquiries to our free Individual Advocacy Service
357
Enquiries received from Western Australians Jan to Mar 2026
Increase in enquiries to our service
23%
Percent increase in enquiries Jan to Mar 2025 v.s. Jan to Mar 2026
Voluntary mental health advocacy need
63%
Increase in mental health cases Jan to Mar 2025 v.s. Jan to Mar 2026
CaLD Cases
36%
Increase in cases for CaLD cases Jan to Mar 2025 v.s. Jan to Mar 2026
Referrals from MHAS and HaDSCO Jan to Mar 2026
31%
Referrals from the the Mental HaDSCO and MHAS
Individual Advocate funding
4.8
We can currently fund only 4.8 F.T.E. Individual Healthcare Advocates.
WA leads Australia
Since the 1990s, the WA Government has demonstrated strong leadership by funding Health Consumers’ Council WA (HCCWA) to deliver a free, person-centred and rights-based service across all areas of health and healthcare. This longstanding investment reflects commitment to a community-led model that restores hope, confidence and power to consumers navigating a complex health.
What is independent individual health advocacy in WA?
Skilled independent patient advocates at HCCWA provide one to one support to a wide range of consumers who need support to have their voices heard, or to get answers when things have gone wrong.
HCCWA provides this support
across the state
across all areas of health and healthcare (including voluntary mental health patients)
across all healthcare settings (public, private, primary, hospital, community)
Individual advocacy impact
Upholds people’s health rights
Enables dialogue between patients and clinicians
Helps to repairs relationships between patients and caregivers where they’ve ruptured
Provides solidarity and encouragement
Restores power and confidence that has been diminished by a large and complex system
Enables redress where things have gone wrong
Saves lives
Independent advocacy provides hope to people at their most vulnerable moments.
HCCWA’s Individual Healthcare Advocacy Service Case Studies
Challenging an unjust $1 million medical bill for a family in distress and holding powerful companies to account
A family coming to Australia to live took out the appropriate level of private health insurance for their visa. Unfortunately, the family needed to access a high level of healthcare. While receiving treatment, the family received a call from their insurance company offering them a different policy with a lower premium, to which they agreed. English is not their first language, and no interpreter was offered. This new policy did not cover the care they were receiving, and so the family became liable for a very significant healthcare bill (over $1m). Our Advocate worked with the family and represented them to the insurance company with the result being that the insurance company agreed to pay the healthcare bill.
Advocate intervention addresses a case of unjust billing
An overseas student was billed for a long GP consultation after a brief visit that lasted around 10 to 12 minutes and included a same day referral to a specialist. The higher charge was more than $100 above a standard consultation and could not be claimed through Medicare due to the patient’s visa status, with private health cover already exhausted. After the patient’s attempts to dispute the charge were unsuccessful, our advocate intervened, referencing the correct billing item requirements. Following several communications, the practice acknowledged the error and rectified the account.
End-of-life choice upheld during fast changing circumstances
“HCCWA was contacted by a family who were concerned that their relative’s rapid health decline was not being adequately recognised and responded to during a hospital admission for abdominal pain. The consumer was subsequently diagnosed with a terminal illness. The consumer decided to access Voluntary Assisted Dying (VAD). Given the conditions that need to be met to remain eligible for VAD, and the consumer’s rapidly declining condition, this case was instantly escalated within our advocacy service. The advocate supported the consumer to seek appropriate and timely clinical reviews, clarify decision-making pathways, and uphold their right to seek and receive clear information. HCCWA’s ability to act quickly ensured the consumer’s preferences, rights, and capacity were prioritised at a critical time.
Restoring quality of life after insisting on surgery review and redress
young man in his early 20s with significant and lifelong disability contacted HCCWA after experiencing escalating pain from a complication following surgery. The procedure differed from what had been discussed and consented to, and post-operative follow up outpatient appointment was not provided. Several GP visits, 2 ED visits and four months later, he still had not received post operative follow up and so remained in severe pain; struggling to access appropriate pain management and unable to resume university study or daily life. HCCWA supported him to understand his rights, be heard within the system, and access urgent post operative review by the surgeon and consider complaint or redress pathways if he chooses. He was admitted for surgery 1 working day after our Advocate spoke with the surgeon.
Western Australians who have used Health Consumer’ Council WA’s FREE Individual Healthcare Advocacy Service (IHAS) say:
“She honestly went above and beyond to help me and make sure I understood everything. Also beautiful and caring as well. ”
“Thank you so much for talking with [clinical specialist] and for helping me prep for my consultation with my doctor and attending with me and writing and sending out the notes. I keep referring back to them as I am trying to fill out the paperwork and pay the fees as I get little blips of panic and they are calming and grounding me massively and that’s allowing me room to actually feel excitement about being on the other side of surgery.“
“Thank you so much for all your help and support in this matter. You truly are amazing and very helpful. It is not often these days you find people that go above and beyond to help you and you truly have so thank you so very much from the bottom of my heart.”
“My advocate was excellent in all areas from knowledge, communication and care to me at all times.”
“Thankyou so much for your time today, I called the right person and I appreciate your help and compassion in a free service too, makes me very grateful I’ve got you and your organisation to lean on for support if I need.”
“Many thanks for all of your support – It has been such a help for me as I was truly so overwhelmed I was unable to do anything and it was impacting my wellbeing tremendously. I cannot thank you enough!!”
“Not only did she guide me in the right direction, she also gave me words of moral support and definitely gave me the confidence to continue the tasks at hand.”
Community led, government funded
A powerful partnership that established Australia’s first independent health advocacy service In 1993, the then Minister for Health offered health consumer leaders the opportunity to set up a non-profit organisation to act as an independent voice for health consumers on all aspects of health and healthcare. The intent had been to advocate at a systemic level for the rights and interests of health consumers, patients and families. Yet when this new organisation was featured in the media, the small team were inundated with requests for help from people who needed answers from the health system about individual issues. And so, those staff started to deliver individual health advocacy “because they couldn’t not”.
Increased investment is now required to ensure this “under the radar” service can continue to be there for every day West Aussies
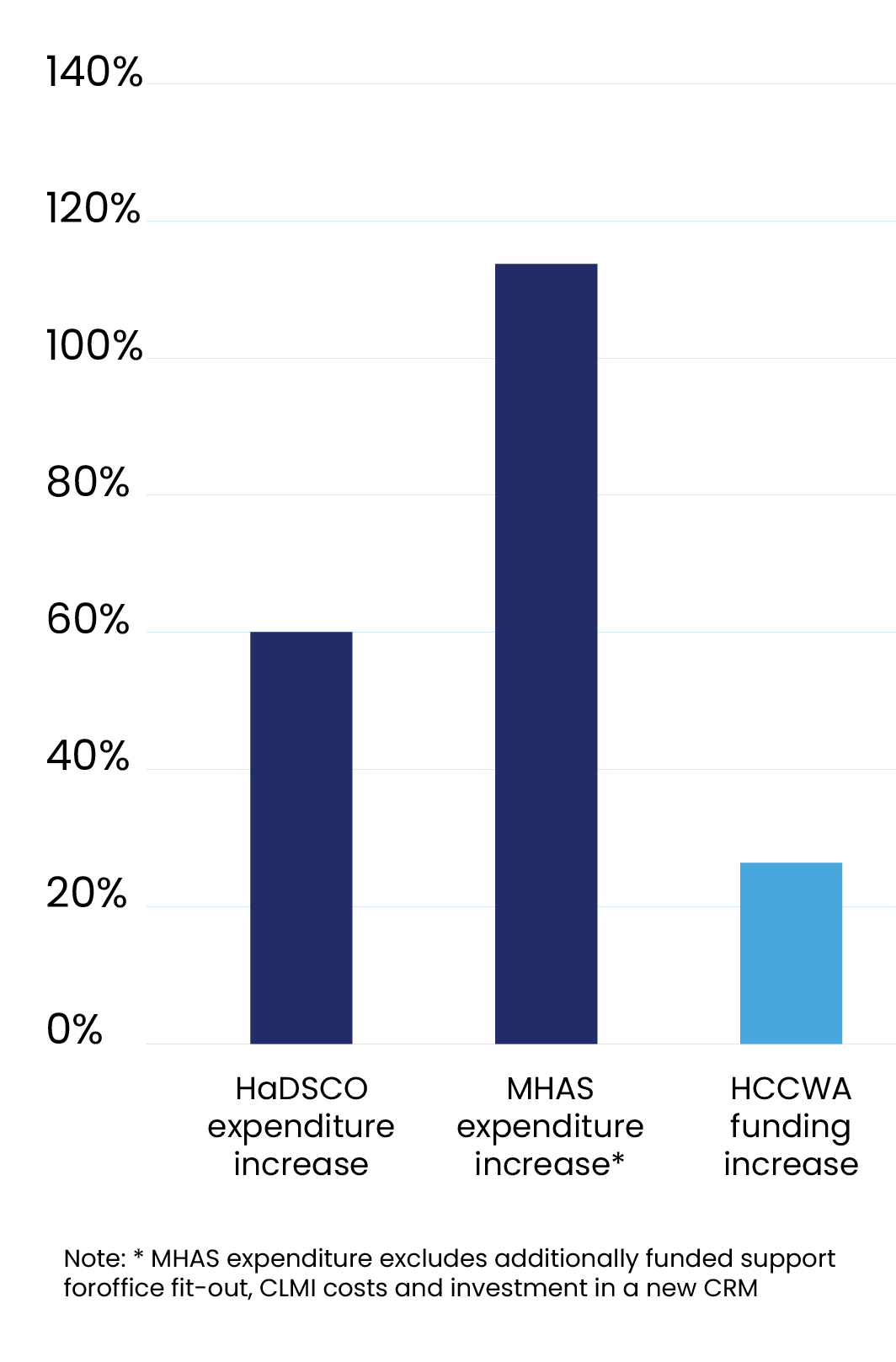
We are in discussions with WA Health about the future of this ground-breaking initiative. After 3 decades, the investment in this service has not kept pace with demand, or with the increased complexity of people’s experiences in healthcare.
Since the HCCWA budget was last reviewed in 2014, WA Health’s budget has increased by 74%, MHAS expenditure has increased by over 110%, but investment in HCCWA’s capacity has only increased by CPI (27%).
We will be seeking support for a budget business case to ensure that this Australia-first program can continue to play its part in the continuous improvement of the health system, and ensure that Western Australians can continue to be heard, respected and supported.
As a minimum, we want to be able to be there for anyone who is involved in a serious clinical incident WA. We estimate that this requires an increased annual investment of $1.9m.
Shifting the dial on patient safety – on-site patient advocates, strengthening consumer voices
Internationally, evidence suggests that approximately 10% of healthcare causes harm. One contributor to this is patients and families being dismissed when raising concerns in a clinical setting. In a busy healthcare setting, patient concerns can go unheard. We believe on-site patient advocates – independent of the WA Health system – would significantly strengthen patient and family voices, enabling their voices to be heard alongside the clinical experts.
This would require a significant phased investment and we would welcome the opportunity to be involved in shaping how this might look for WA.
For further information about this report please contact Health Consumers Council WA on 08 9221 3422 or info@hconc.og.au
To discuss any of the content, please contact Clare Mullen, Executive Director at CEO@hconc.org.au
Health Consumers’ Council WA’s latest Systemic Advocacy Report highlights how consumer and community voices are helping shape health policy, services, and system reform across Western Australia. Covering January to March 2026, the report outlines HCCWA’s work across preventative health, referral pathways, consumer engagement, rural access, Aboriginal health, mental health, and informed decision making.
During this period, HCCWA contributed to policy submissions, Ministerial roundtables, committee governance reviews, and national reform discussions, while continuing to bring lived experience perspectives into high level decision making. The report also highlights advocacy on outpatient access, informed financial consent, consumer rights, and the need for more inclusive and community-led approaches across the health system.
The report reflects HCCWA’s ongoing commitment to ensuring healthcare policy and reform are shaped by the experiences of patients, carers, families, and communities across WA.
Acknowledgements
We acknowledge Aboriginal and Torres Strait Islander peoples and communities as the Traditional Custodians of the land we work on, specifically the Whadjuk people of the Noongar nation, and pay our respects to Elders past, present, and emerging. Australia always was and always will be Aboriginal land.
Health Consumers’ Council acknowledges the unique insights and strength of those who navigate the complexities of the health system as consumers and thank them for sharing their lived experience and wisdom to help make healthcare fair for everyone.
In this report we provide our members, friends and stakeholders with an update on how we’re amplifying and championing diverse consumer and community interests to help drive positive change across the health and social care sectors in WA.
During this period, HCCWA continued to influence policy, strengthen partnerships, and elevate consumer and community voices across the health system.
Our reach and engagement
Contributed to 5+ policy submissions and strategic consultations
Engaged with state and national government agencies, Ministers and MPs
Participated in 10+ committees, advisory groups, and sector forums
Delivered 3 sector presentations and panel contributions
Contributed to media coverage on key consumer health issues
Key areas of influence
Preventative health policy and whole-of-government approaches
Access to care, including referral pathways and rural primary care
Consumer engagement and lived experience in system design and governance
Equity in health care, including Aboriginal health and community-led approaches
Transparency and informed decision making for consumers
Highlights from this period
Provided strategic input to the WA Department of Health Capability Review, strengthening the focus on consumer and community partnership
Contributed to national policy discussions on modernising referral pathways, advocating for improved access, transparency, and informed choice
Supported Ministerial roundtables on preventative health, bringing forward consumer priorities including early years, social determinants, and community-led approaches
Facilitated engagement between Aboriginal Elders and the Minister for Health and Mental Health, elevating community perspectives on research and program design
Shared insights across sectors, including presentations to the WA Country Health Service and the Community Relief and Resilience Network
This work reflects HCCWA’s ongoing role in ensuring that consumer and community voices inform policy, shape services and contribute to a more equitable and responsive health system.
How systemic advocacy is organised at HCCWA
This period we said farewell to Bronwyn Ife, HCCWA’s Systemic Advocacy Lead, who returned to a role in local government. As the fixed term funding that covered the Systemic Advocacy Lead role is not ongoing we will not be replacing that role. Due to funding constraints, HCCWA’s systemic advocacy work is undertaken by members of the Leadership team alongside their other responsibilities.
Do you find this information valuable?
This is a new publication for us, and we’d welcome feedback – what is helpful/interesting? What is not?! Let us know by emailing us at engagement@hconc.org.au
HCCWA was approached as a key stakeholder to provide input to inform the Capability Review of the WA Department of Health. These reviews are carried out by the WA Public Sector Commission as “a permanent, ongoing mechanism to lift the capability of the public sector and drive performance improvement”. HCCWA’s feedback covered WA Health’s approach to partnering with consumers and the community.
HCCWA was approached for preliminary feedback about proposals to review specialist titles in dentistry. HCCWA’s feedback was:
The language and formatting of these consultation materials is very complicated and likely to be challenging for most consumers/community members – unless they’re very experienced consumer representatives, or work for a consumer organisation.
This is a very important topic – we know that some of the harm that’s been experienced by consumers in recent high profile cases is due to the lack of clarity about the different abilities of general dentists and prosthodontists
Ahpra and the Dental Board should seek targeted input from consumers across the country
Attention should also be paid to how consumers are informed about these distinctions, how consumers can be sure they’re being treated by someone with the appropriate skill level and qualifications, and how they can make informed choices about which health professional they choose to be treated by.
We highlighted the benefits of hospices and the important role they can play in supporting patients and families both in the community as people live with life-limiting conditions, and at end of life.
We highlighted the importance and value of the Compassionate Communities approach, including the evidence about their value in reducing hospital use from the South West: research from 2023 showed lower hospitalisations, less hospital days/month, and less emergency presentations https://journals.sagepub.com/doi/epub/10.1177/26323524231205323)
Australian Department of Health, Disability and Ageing
This consultation sought the views of patients, medical providers and other interested parties on whether current Medicare referral arrangements are effectively supporting access to specialist care. It also seeks views on suggestions for reform.
HCCWA provided this feedback:
The current referral process does not make it easy for patients to access specialist care
Including cost information and links to Medical Costs Finder on referrals would help patients make more informed financial decisions
Patients should be able to switch specialists under the same referral without needing a new referral
Our GPs should be kept informed about our treatment with the specialist throughout the duration of the referral – if that is what we want
The lack of information available to consumers to make truly informed decisions about their preferred referral options could be a barrier to the take up of an Australia-wide digital referral process.
There is almost no information consumers can use to determine the quality of care they might receive for any particular clinicians. For communities who are often served by overseas trained doctors, their treating doctor may not have any knowledge or pre-existing relationships with other clinicians to inform their recommendation.
This could be addressed by requiring clinicians to publish information about any complaints they receive (noting that not all consumers have the emotional energy to go through the administratively heavy Ahpra notification process). Or to strengthen the Ahpra annual registration process to require evidence of consumer feedback in some way. While google reviews may be inadequate, they are sometimes the only publicly available information for consumers to use as they try to make an informed decision.
It is important that consumers are able to access neutral information about things to consider when looking for a specialist. The “service” is highly technical, and the “market” is diffuse and confusing to navigate. There’s a risk that “good bedside manner” could become the standard for decision making in the absence of consumers being able to access other information about other quality measures they could consider.
That any policy should be supported by significant investment in ensuring consumers are supported to make fully informed decisions. For example, all referrals could be required to include mandatory wording directing consumers to online information about how to make a decision, and what questions to ask about their options.
Information about making informed decisions should be co-designed by consumers, and could be included in consumer-led training delivered by consumer organisations.
Recent media accounts – Four Corners – have made it very clear that our healthcare system cannot be based on doctors policing themselves. While many are trustworthy people who deliver high quality care, it is clear that where this is not the case, the consumer has little hope of receiving honest feedback about colleagues from their own doctors.
Mandating the provision of information in plain language that has been written by consumers for consumers that outlines the process, their rights, and what they can expect – i.e. informed financial consent – and where to go if they have questions could improve patient understanding of referral arrangements. This could be on a website – similar to the Choosing Wisely program.
The ability for patients to seek a second opinion from a new specialist under the same referral would be enormously beneficial for patients. In the current “market” consumers are significantly disadvantaged and disempowered by limited access to information on which to base their decisions. Being able to access a second opinion is likely to have a significantly positive impact.
If were to be coupled with powerful AI-powered consumer healthcare decision tools, this will be a game-changer in terms of re-empowering consumers.
HCCWA was one of the signatories to a letter seeking an update on the implementation of the recommendations from the Statutory Review of the Mental Health Act 2014 (WA) that was completed in 2024.
As background, HCCWA contributed to the Review in 2021 by hosting consumer consultations on the experiences of people accessing mental health services on a voluntary basis. We look forward to being able to share how these recommendations are being implemented with our community.
HCCWA was asked to review draft guidelines for WA Health staff on establishing and running committees.
Our feedback related to how to ensure that including consumer, community and lived experience voices in WA Health committees was a valuable experience for everyone.
HCCWA’s Executive Director, Clare Mullen, took part in a Leadership Discussion Circle with a group of WA Country Health Service leaders, sharing HCCWA perspectives on partnering with consumers at all levels of decision making.
Clare Mullen presented to the Community Relief and Resilience Network on key health consumer issues, contributing a consumer perspective to discussions across the emergency relief sector.
The Community Relief and Resilience Program provides policy representation and sector support to Western Australia’s emergency relief sector. These services support individuals and families experiencing poverty or financial stress through food and material aid, financial assistance and referrals to other support services.
There are more than 300 agencies across WA delivering community relief, ranging from small volunteer-run services to large multi-program organisations.
Tania Harris, HCCWA’s Engagement Manager, Aboriginal and Torres Strait Islander Lead and Disability Lead, took part in a panel discussion that brought together perspectives from research, consumer advocacy, clinical practice, innovation and policy.
The panel explored whether current policy, funding and service delivery frameworks are fit for purpose and effective in translating diabetes innovation into equitable care with HCCWA contributing a consumer and lived experience perspective to support more inclusive and responsive approaches.
The Hon Sabine Winton MLA, Minister for Preventative Health
HCCWA attended four preventative health roundtables at the start of 2026:
Mental Health and Early Years Wellbeing
Health Promotion
Screening and Genomics
Immunisation
Across all of these sessions we shared what we hear from consumers, carers, family and community members:
Need to address the social determinants of health, particularly poverty/low-income
A focus on first 1,000 days and healthy families is essential – particularly preventing and addressing early childhood trauma
A lot of prevention takes place outside the “health system”; Government needs to be joined up in its approach
There is a need for more community-driven/community-led health promotion activities at a place level
Need much more involvement of a wide range of consumers, carers, families and people with lived experience in all scoping, planning, delivery and evaluation of initiatives
Targeted work should be done to include the voices of people who may not engage in traditional “consultations”, including people experiencing homelessness, people with intellectual disability, and people where English is not their first language
The value of peer-led approaches across all areas of health and mental health – including in health promotion activities within and outside clinical settings
The Hon Meredith Hammat MLA, Minister for Health and Mental Health
HCCWA supports the Healthy Lifestyle Program’s consumer engagement and directly supports and facilitates the Healthy Lifestyle Program Cultural Advisory Group and its members (the Elders). The group is made up of respected Aboriginal Elders who have decades of experience supporting researchers and research projects.
The Elders were concerned about the impact of short-term research pilots on their families and communities. They requested the opportunity to meet with senior decision makers to share their and their communities’ perspectives and experience with the research pilot pathways.
Minister Hammat and her team met with the Elders in March 2026 and welcomed the opportunity to hear about the program and their experience.
Since 1994, Health Consumers’ Council WA has been advocating for the interests of the WA community, health consumers, patients, carers, and families when it comes to health and healthcare.
HCCWA will continue to work across government, the health system, and the community to ensure that consumer voices shape policy, services, and system reform. This work remains critical to building a more equitable, responsive, and person-centred health system in Western Australia.
For further information about this report please contact Health Consumers Council WA on 08 9221 3422 or info@hconc.og.au
To discuss any of the content, please contact Clare Mullen, Executive Director at CEO@hconc.org.au
WA is the first state to have a Minister for Preventative Health, the Hon Sabine Winton. Late last year, Health Consumers’ Council WA was invited to be part of a number of roundtables gathering input to inform the development of WA’s first preventative health strategy.
There were six roundable discussions and HCCWA were invited to attend four:
Mental health and wellbeing in the early years
Immunisation
Health promotion
Cancer screening and genomics
The other two were:
Sexual health
How government departments work together on this agenda
A number of other consumer and community organisations attended some of the sessions including Alcohol and Other Drug Consumer and Community Coalition, WA Association for Mental Health and Aboriginal Health Council WA.
HCCWA’s input to these discussions was based on the deep and broad understanding of health consumer interests which comes from our daily interactions with patients, families and carers, people with lived experience and community members. In general our input was:
It’s critical to address the social determinants of health – particularly poverty.
A focus on the first 1,000 days and healthy families is essential – we highlighted the need to have a concerted focus on preventing and addressing early childhood trauma
A lot of prevention takes place outside the “health system”; Government needs to be joined up in its approach, and move to being more community-centred, and less “service-centred”
There is a need to invest in more community-driven/community-led health promotion activities at a grassroots level
Unsurprisingly we called for much more involvement of a wide range of consumers, carers, families and people with lived experience in all scoping, planning, delivery and evaluation of all preventative health initiatives
Targeted work should be done to include the voices of people who may not engage in traditional “consultations”, including people experiencing homelessness, people with intellectual disability, and people where English is not their first language
The value of peer-led approaches across all areas of health and mental health – including in health promotion activities within and outside clinical settings.
The Minister sat in the room for the duration of each session and I had a clear sense she’d listened deeply and took the feedback on board. She also made reference to a public facing consultation process – we’ve flagged with her office that we’d like to work with them to ensure wide and deep engagement.
We’ll circulate more information about the public consultation when we get it. Clare Mullen, Executive Director
Western Australia Health Systemic Advocacy October to December 2025
We acknowledge Aboriginal and Torres Strait Islander peoples and communities as the Traditional Custodians of the land we work on, specifically the Whadjuk people of the Noongar nation, and pay our respects to Elders past, present, and emerging. Australia always was and always will be Aboriginal land.
Health Consumers’ Council acknowledges the unique insights and strength of those who navigate the complexities of the health system as consumers and thank them for sharing their lived experience and wisdom to help make healthcare fair for everyone.
Since 1994, Health Consumers’ Council WA has been advocating for the interests of the WA community, health consumers, patients carers, and families when it comes to health and healthcare. That work involves maintaining productive relationships with a wide range of people across health and social care so that consumer interests influence every level of decision making. Much of this work is done on a daily basis behind the scenes. We want to provide our members, friends and stakeholders with a regular update on how we’re amplifying and championing diverse consumer interests to help drive positive change.
This is a new publication for us, and we’d welcome feedback – what is helpful/interesting? What is not?! Let us know by emailing us at engagement@hconc.org.au
Met with the Network of Consumer Representatives across WA Health Services and discussed the systemic advocacy program with them
Attended the launch of the WA Council of Social Services (WACOSS) budget submission and AGM
Attended the launch of the Justice Through Our Eyes, 100 Voices for Change report
Met with WA Health Department staff to discuss consumer involvement in health infrastructure projects
Discussions with WA Health Senior staff on increasing access to individual advocacy
Met with WA Health to discuss the contracts in place around hospital parking costs
Discussed the refreshed Outpatients Strategy with Department of Health Staff
Attended the launch of the St John Ambulance Impact report
Attended two meetings with the team from Care Opinion while they were in Perth, and discussed an upcoming event
Met with Frank Paolino, member for Mt Lawley, to introduce HCCWA and our work
Met with Dan Bull, member for Bayswater, to introduce HCCWA and our work
Attended the Behind Bars Beyond Care panel event hosted by the WA Justice Association to hear stories of the prison health system and how it impacts the lives of incarcerated people
Attended the Joint Commissioning statewide forum, hosted by the Commonwealth Department of Health, WA Primary Health Alliance, the State Department of Health and the Aboriginal Health Council of WA to discuss opportunities for collaborative commissioning projects across the health sector
Quarterly meeting with the Director General of the Department of Health
Met with staff from the Department of Health to discuss progress on the consumer involvement on the new Women’s and Babies’ hospital. Raised the issue of affordable parking access among other things.
Met with the DOH staff member involved in the management of the state dialysis services contract to discuss contract KPIs and consumer concerns
Met with the CEO of the RRR Network – network of Regional, Rural and Remote women, to discuss shared interests and ensure they know how to promote regional interests through HCCWA’s work.
While this inquiry was initially inspired by the public response to building the motor racing track at Burswood Park, the Terms of Reference were broad and included the ability to discuss planning laws broadly. We’re always on the lookout for opportunities to raise community concerns with key decision-makers, so we grabbed this chance to talk about Fast Food restaurants in planning laws.
We shared the following:
Currently there is no consistency in planning laws around the classification of fast food restaurants. Some Local Governments classify them as a “restaurant” while others classify them as “takeaway facility with drive through”.
Having a separate category for fast food/junk food venues would allow Local Governments to prevent fast food vendors from operating in certain areas, such as near primary schools.
The current categorisation as “restaurant” means that in some locations there are fast food establishments close to schools and close to other restaurants that offer fresh and healthier food options that may be more expensive than fast food.
This contributes to children being exposed to fast food advertising, and research tells us that children are heavily influenced in this way, and that exposure to fast food establishments and advertising contribute to unhealthy eating and rising obesity rates.
Having a category in planning law specifically for fast food establishments would provide Local Governments with the statutory framework they need to ensure that these establishments are only approved in more appropriate areas, away from schools and away from healthier food options.
The Department of Justice Clinical Governance Advisory Group considers policies within the justice system that relate to health care. This policy allows for prisoners to make private Medicare appointments in some circumstances where the services that they require are not available to them in the prison system. The policy focused heavily on the practicalities of making appointments and transporting patients to and from those appointments. We felt that there were some gaps in the policy that needed to be clearer.
We shared the following:
There was no indication of what criteria are used when approving requests for private appointments. We recommended that these be clearly stated.
There was no clarity around the sort of appointments that might be sought by patients. For example, there might be circumstances where an appointment is available in the justice system but the patient would prefer a specific practitioner, and is able to pay for such an appointment. We asked that the policy make it clear on whether these private appointments do allow patient choice or if they are only to be used for services that are clinically necessary but unavailable in the justice system.
We also asked for clarity on what happens when a patient needs treatment that is not available in the justice system but is unable to afford a private appointment.
There was no information in the policy about patients appealing a decision made under that policy. We argued that this should be included.
This matter came to our attention when we attended a forum on healthcare in the prison system. We heard a social worker speak who told us that when women who are in the justice system deliver babies who are either pre term or need special care for other reason, they are then separated from those babies for extended periods of time once the mother is well enough to be discharged. The baby remains in the care of the hospital while the mother returns to the prison system and the capacity for the baby and mother to spend time together is heavily restricted. This is a human rights issue, and also surprising in the context of the recent focus on the first 1000 days of the life of a baby. This policy was not yet scheduled for review by the committee, but we asked to provide some thoughts.
We shared:
The current policy that covers pregnancy is missing any information on what happens immediately after the birth of the baby
The policy seems to assume that the baby will be well enough to be discharged at the same time as the mother, but even then there is no information given about the expected procedures to follow with where the mother and baby will be accommodated.
We asked what arrangements are able to be made and what policy considerations can be put in place for a mother and baby to spend crucial time together when the mother is well enough to be discharged but the baby is not.
There are studies that confirm that women in the prison system are more likely to give birth to pre term babies, due to a combination of factors. Given that pre term birth is a specific risk for the population served by this policy, it is important that the policy addressed those circumstances.
We also noted that the policy is silent on high risk pregnancies, such as those where a mother needs to on extended bed rest or is at an elevated risk of pre eclampsia.
The Department of Justice shared their Deaths in Custody policy for feedback. This policy was mostly focused on managing the scene following a death in custody.
We shared:
That such a policy should also include information about informing and supporting families following a death in custody
We asked if the partner policy which applied to Youth Detention Centres, which we had not viewed, was the policy that covered Unit 18 at Casuarina Prison as well.
The policy has a section on what occurs when a patient dies outside of a custodial facility. We asked if this section could also include information about how it is determined if the patient’s status as a prisoner had contributed to their death – for example were restraints used that may have meant that their experience was different to the experience of a patient who is not a prisoner.
The policy did not elaborate on the training, resources, capacity and medication available to staff to undertake a full resuscitation, so we were unable to learn from the policy if staff are able to resuscitate a patient or rather continue to provide CPR until an ambulance arrives.
The McCusker Centre for Citizenship at UWA runs a program where students undertake internships with organisations as part of a their university studies. We have hosted a number of McCusker interns who have undertaken a variety of projects for us. We were invited to sit on a panel at a McCusker Alumni event to talk about the health system in WA. This was a great opportunity to speak to students who were mostly studying degrees in health and to help them understand the health sector through a consumer lens. We discussed workforce issues in rural and remote areas, health rights, preventative health and programs that help people stay well, in their communities and out of hospital. We talked about how your postcode can influence how healthy you are and how long you live. For some of these students this was a whole new experience and a new lens through which to understand their chosen field of study.
Monthly meetings with Systemic Health Advisory Collective – a group of systemic health and policy staff from WA Based consumer organisations in the Mental Health space.
Interview with Seven West media about the HaDSCO Annual Report data – highlighting the limitations of the health complaints process, and the role that independent advocates play to support consumers
Interview with Choice Magazine on issues around early release of superannuation and upfront payments for costly dental treatment
ABC Perth Radio and ABC news – interview on the State Government’s $1.5 billion investment in hospital infrastructure, welcoming the investment and reiterating the need for investment in preventative health.
For further information about this report please contact Health Consumers Council WA on 08 9221 3422 or info@hconc.og.au
Health Consumers’ Council WA calls for urgent action to address GP access and affordability in WA
The latest Cleanbill Blue Report reveals a mixed picture for Western Australians seeking GP care. While the national rate of fully bulk billing clinics has doubled to 40.2%, Western Australia lags far behind at just 19.8%, the second-lowest rate in the country. At the same time, out-of-pocket costs for those not bulk billed have risen to an average of $46.63, up nearly 10% from last year.
Health Consumers’ Council WA Executive Director Clare Mullen said these figures highlight a growing equity gap in primary care access across the state.
“Western Australians deserve timely, affordable healthcare, yet these findings show that too many people are still facing significant barriers. Bulk billing remains the exception rather than the norm in WA, and rising costs risk pushing care out of reach for those who need it most.”
The report also notes a national trend of GP clinic closures and consolidations, raising concerns about future availability of services in regional and remote WA.
“Consumers tell us every day about the stress and hardship caused by limited access to GPs. We need urgent, coordinated action to ensure that incentives translate into real improvements for WA communities—not just on paper.”
Health Consumers’ Council WA is calling for:
Greater transparency on GP pricing and availability.
Targeted support for clinics in WA to adopt bulk billing practices.
Consumer voices at the centre of policy decisions to ensure reforms meet community needs.
As an independent organisation advocating for health equity, HCCWA will continue to amplify consumer experiences and push for solutions that make healthcare accessible for all Western Australians.
ENDS
Media enquiries: 0488 701 839 | info@hconc.org.au
Bronwyn Ife | Systemic Advocacy and Engagement Lead
From the desk of HCCWA Executive Director, Clare Mullen
HCCWA x Healthway
Today I caught up with Carina Tan-Van Baren, Executive Director of Healthway. Healthway plays a vital role in keeping Western Australians healthy by investing in prevention, community wellbeing, and health promotion.
Our conversation focused on the role of health consumers and community members in shaping Healthway’s future work. As with all parts of the health system, we discussed the importance of consumer involvement at every level of decision-making — including at board level.
We chatted about opportunities to strengthen grassroots, community-led prevention, including Compassionate Communities, “staying in place” initiatives, and other place-based approaches that support people to live well where they are. We also discussed the potential for prevention work in Western Australia to place a stronger focus on preventing and addressing the impact of adverse childhood experiences.
It was also a chance for us to share the work we’ve has been doing since 2018 — supported by WA Health and WAPHA — on The WELL Collaborative.
Strategies for Action from the WA Healthy Weight Action Plan: “a community that supports maintaining a healthy life”
This is WA’s innovative approach to bringing together people with lived experience with academics and health practitioners to help shape policy and system change to achieve the vision of the WA Healthy Weight Action Plan: “a community that supports maintaining a healthy life”
It was a very productive conversation about the opportunities for lived experience perspectives to be front and centre when thinking about health promotion. We’ve agreed to keep meeting regularly over the coming year — so watch this space.
We are currently in the middle of 16 Days in WA 16 Days in WA – an event that runs from between the International Day for the Elimination of Violence against Women on 25 November to World Human Rights Day on 10 December. Family and Domestic Violence is a key Social Determinant of Health, and the majority of people who experience this violence are women, with 2 in 5 women experiencing violence since the age of 15 and one women killed every 9 days by a current or former partner.
men’s control of decision-making and limits to women’s independence
rigid gender stereotyping
cultures of masculinity that emphasise aggression, dominance and control
The impact of gendered violence is devastating and far reaching. As well as being a leading cause of homelessness for women, intimate partner violence contributes to more death, disability and illness in women aged 25 to 44 than any other preventable risk factor.
The impact of violence against women is seen in workplaces as it affects staff retention, absenteeism, productivity and morale. Violence against women in Australia is believed to cost Australia $21.7 billion each year.
When we attended the WA Health Awards on 25 November, we were thrilled to see the recognition given to the program at North Metropolitan Health Service for Clinical Awareness and Response Enhancement for Family and Domestic Violence. This initiative was co-designed with victim-survivors and introduced ED-specific clinical pathways, confidential disclosure processes, and a multidisciplinary education program. This has led to a 68% increase in victim-survivors engaging with safety planning and social work. It also improved medical documentation and enhanced the overall care experience for those affected by Family and Domestic Violence.
At HCCWA we are committed to anything that improves the health and wellbeing of our community. Tackling the gendered drivers of violence, and addressing violence against women are key steps to contribute to a safer, healthier community.
Health Consumers’ Council WA (HCCWA) welcomes today’s announcement by the WA Government of increased investment in hospital capacity, recognising it as an important step in responding to the current demand for hospital care.
HCCWA Executive Director Clare Mullen said the investment would be reassuring for people struggling to access timely care, and emphasised that the ultimate goal must be a healthier population that requires less hospital care in the first place.
“Every Western Australian deserves access to high-quality hospital care when they need it —but a truly sustainable health system keeps people healthy and supported before they reach crisis point,” Ms Mullen said.
“No one wants to need hospital care. Ill-health need not be inevitable. To reduce pressure on hospitals, we need to invest just as strongly in prevention, early intervention, and the social conditions that keep people well.”
Ms Mullen said consumers consistently raise concerns about the difficulty of accessing affordable and timely primary and community care and early intervention with health issues —particularly for people living with or at risk of chronic conditions, or in regional and remote areas.
“When there is a lack of early intervention programs, or people can’t access the right care at the right time, health problems escalate and hospital admissions become inevitable,” she said.
“It’s a relief to see hospital expansion to ease the current pressure on services. But without strong community-based options, as well as targeted investment in preventative health activities, the demand for acute care will keep rising.”
“Western Australians want to see a system that supports health, as well as one that treats illness — one that helps people to stay well, connected and supported in their communities.”
HCCWA is calling for a balanced approach that includes:
Long-term investment in early intervention and preventive health programs,
Better funding for community-based and multidisciplinary care, and
policies that address the social and economic drivers of poor health.
“This is a welcome and necessary investment in hospital capacity. And we look forward to partnering with WA Health to ensure consumers and community members are actively involved in shaping these important infrastructure projects,” Ms Mullen said. “And if we want fewer people needing hospital care, we must also invest in prevention.”
Joint AHPRA and ATO Statement Targets Predatory Dental Payment Practices
We’ve seen time and again that consumers speaking up can drive change, and last week was no exception. Consumers who have been impacted by poor practices by WA dentists have collaborated with HCC and together we are we are making changes.
We celebrated a victory last week when APHRA and the ATO issued a very strong joint statement on the worrying misuse and overuse of the compassionate release of superannuation to pay for dental treatment. The agencies gave strong guidance to practitioners on the limited circumstances in which it is appropriate to use such payment methods and also undertook to investigate practitioners who they believe are using this system inappropriately.
Unlike previous statements on this topic, which were framed as partly a caution to patients, this statement places the responsibility squarely with practitioners and with third party agents who may assist in completing applications for early release of super. We welcome this change in approach, and we are really pleased that these regulators have listened to consumers and to our advocacy in framing this message.
We heard about this issue earlier this year, following the death of a dental practitioner who had taken substantial advance payments from patients for expensive dental treatment, but had passed away before delivering the treatment.
In our research, we found a worrying number of practitioners who include in their advertising materials information that encourages people to withdraw their superannuation to pay for treatment. Some of this advertising appeared predatory and was often included incorrect information.
After advocacy from us, in partnership with consumers and pressure from the media, there was a press release from AHPRA in late May which expressed concern about the increase in using superannuation to pay for treatment, and a great checklist of red flags for consumers. This was a pleasing start, but we continued our advocacy, as we were concerned that the messaging from regulatory bodies around this practice was not strong enough.
The statement issued on 16 October is strong. It speaks of inaccurate statements being made by practitioners on forms supporting the release of superannuation, and of the penalties that people will face for making such statements. The consumers who have been left stranded are continuing their fight for justice through legal avenues, the media, and complaints processes. We are continuing to work with Consumer Protection, AHPRA and Choice Australia to explore avenues to protect consumers in future.
Bronwyn Ife | Systemic Advocacy and Engagement Lead