We have collected or developed the below resources to help newly arrived migrants, people who are unfamiliar with the WA health system, and/or those who do not have English as a first language. Not all resources are available in languages other than English, but where available we have provided links.
Covid-19 multicultural resources – A collection of Covid resources in languages other than English from both government and reputable other organisations. Includes a video about the government’s COVIDsafe app available in 8 different languages and also a link to download a Covid information app in language.
Overview of the WA Health System – This Government of WA, Department of Health page gives a brief overview of the WA public health system and how it is divided up (geographically) into the metropolitan services of North Metropolitan Health Service, The South Metropolitan Health Service and The East Metropolitan Health Service plus the The Child and Adolescent Health Service and WA Country Health Service for regional and remote. Links to each of these services are provided on the page.
Medicare eligibility and enrolling – This Australian Government page explains who is eligible for Medicare and how to enrol for a Medicare number / card.
About Medicare – This Australian Government page explains what is covered by Medicare and how to make claims (for money back or rebates)
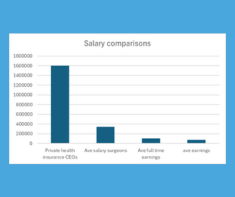
Choosing Private Health Insurance – This page by the Commonwealth Ombudsman for Private Health Insurance explains how private health works in Australia and provides information on choosing a policy.
Your healthcare rights – This Health Consumers’ Council page explains your (legal) rights in healthcare around informed consent and the right to competent care. Links also to more detail about mental health rights.
Going to hospital – Easy English Version – This is a Health Consumers’ Council produced brief brochure which explains (in simple English with few words and plenty of images) what to expect if you are going to hospital. Includes what to pack and a bit about what to expect when you get home.
Going to hospital – Languages Other Than English – The above mentioned Health Consumers’ Council brochure is available in Farsi, Arabic, Urdu, Dari and Karen.
Choosing the right health service – This animated video from Health Direct (available in English, Arabic, Bengali, Chinese and Vietnamese) explains when it’s appropriate to use an online information resource, consult a telephone or online health help line, consult a pharmacist, consult your GP or go to hospital.
The role of a GP – This animated video from Health Direct (available in English, Arabic, Bengali, Chinese and Vietnamese) explains the role of a General Practitioner (GP) or local, family doctor. It explains what a GP can do for your and your family and how and when they will pass you over to a specialist doctor. It explains how to find, choose and access a GP.
Paying for Healthcare – This animated video from Health Direct (available in English, Arabic, Bengali, Chinese and Vietnamese) discusses the cost of various health services and what services are covered by Medicare, the government scheme that helps Australians pay for healthcare.
Maternity Services – This animated video from Health Direct (available in English, Arabic, Bengali, Chinese and Vietnamese) looks at options for pregnancy care and where to give birth in Australia and the costs associated with the services.
Baby’s First Weeks – This animated video from Health Direct (available in English, Arabic, Bengali, Chinese and Vietnamese) looks and the services and support you can receive in the weeks post birth of a baby when living in Australia.
Mental Health – Link to the Embrace Multicultural Mental Health portal which is for both community and services providers. For community there is a range of mental health resources in multiple languages as well as some personal stories and a list of community support organisations.
Five Questions To Ask Your Doctor – This is a Choosing Wisely provided resource, available in multiple languages, which provides five (5) questions which it is sensible to ask your doctor before opting for any test or treatment (together with a brief explanation as to why each is important).
Speaking Up and Giving Feedback – Link to the Health Consumers’ Council page of “self-advocacy” resources. It provides key resources and links to websites to support yourself in the health system, and provide feedback to our health services.
The Health Translations Directory – A Victorian Government library of health resources which have been translated into multiple languages. A very well stocked library which you can search via topic / condition or via language.
If you are from a Culturally and Linguistically Diverse (CaLD) background or work with people from a CaLD background then please participate in our survey on available health literacy resources for CaLD populations.
Click here to complete the survey